Consolidation | Complex effusion | Empyema | Fibrosis | Interstitial syndrome | Pneumothorax | Pleural effusions | Rib fracture
Consolidation
Pneumonia on ultrasound can be seen as a variety of signs – from unilateral B lines in the BLUE protocol to a hepatized lung seen when the parenchyma are densely consolidated. Various examples are shown in the video below.
| Back to top
Complex pleural effusion
The video belows shows a complex, loculated pleural effusion. This is almost undoubtedly a transudate, but drainage may be limited by the septae causing pockets of fluid. It would be senisble to place a medium bore drain (12Fr or above) if you see these appearances and are planning for a pleural drain.
| Back to top
Empyema
An example of an empyema is shown below. Note that many empyema will appear as simple effusions only and you cannot use ultrasound appearances to confirm or refute the diagnosis – the fluid must be sampled if clinical suspicion is present.
| Back to top
Fibrosis
Pulmonary fibrosis is often thought sonographically to appear as B lines throughout the affected portion of lung. This video demonstrates that is not always the case, as fibrosis may also show an irregularity to the pleural line without clear evidence of B lines. In this video you can also see thickening of the diaphragm (consistent with chronic respiratory failure), and heterogeneity to the ventilation of the lung (evidenced by varying degrees of lung sliding). None of these features are pathognomonic, but put together they may indicate fibrosis as in this case.
| Back to top
Interstitial syndrome
The video below demonstrates the appearance of the interstitial syndrome on ultrasound. In medical practice, this will often represent pulmonary oedema. As you can see from the BLUE protocol pages, however, you may also see these appearances due to pneumonia, and ARDS and lung fibrosis may also generate the B lines seen here.
| Back to top
Pneumothorax
This video shows the ‘lung point’, the pathognomonic sign of pneumothorax (ie 100% specific). The lung point is the point on the chest wall where the air lifts the visceral pleura from the parietal pleura and so you see a combination of lung sliding (pleura opposed) and no lung sliding (pleura separated).
The other feature seen in pneumothorax is an absence of lung sliding (and no B lines – a B line would categorically rule out pneumothorax). An example of this is seen below. Again, it is important to note that absent lung sliding can be seen in a number of conditions and so is not diagnostic of pneumothorax.
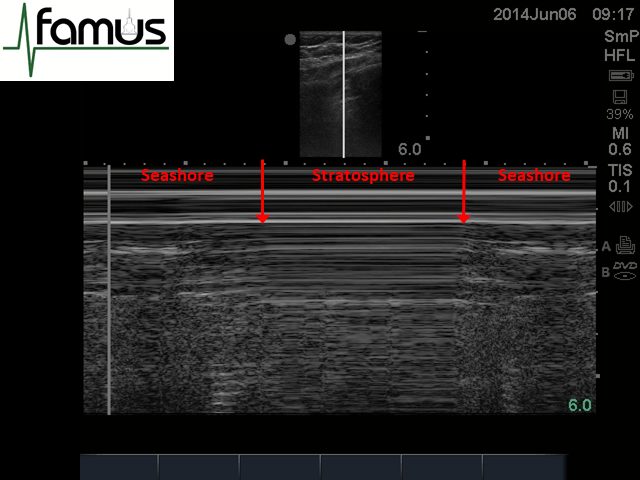
As you can see from the theory section, the presence of a pneumothorax on M mode will elicit a ‘stratosphere’ sign. The image below shows what an M mode image looks like through the lung point, where you can see the seashore sign either side of the stratosphere sign (boundaries marked by red arrows). The video below this image gives another example of the lung point and appearances of M mode through it.
| Back to top
Pleural effusions
The video below highlights some of the different types of pleural effusion which can be visualised on ultrasound. It is worth noting that if septations are seen prior to inserting the drain, you may wish to consider a Seldinger drain rather than the newer cannula-like drainage kits. You may then use the guide wire to try to break some of the septae prior to drain insertion. Similarly, if the fluid looks proteinaceous it may influence you to use a larger bore drain and/or regular flushes to reduce the chances of it getting blocked.
| Back to top
Rib fracture
Ultrasound examination of bones has recently started to gain favour, and this video shows how ultrasound can diagnose a rib fracture quickly and easily. In this case, the fracture was the left lateral 11th rib, an area that would not be visible on routine CXR. By placing the probe at the maximal point of rib tenderness you can quickly ascertain if the periosteum is intact and therefore whether a fracture is present.
| Back to top